

About Us
The Vein Institute of Hunterdon
The Vein Institute is proud to be accredited by the Intersocietal Accreditation Commission (IAC). Our primary focus is on our patients and their comfort, providing the highest level of vascular and aesthetic care to the Hunterdon and Somerset communities. We strive to ensure every patient experiences a relaxed, professional environment from the moment they walk through our doors.
Founded and led by Dr. Glen Tonnessen, a board-certified cardiologist with over three decades of medical experience, our team of highly skilled health care professionals provides progressive state-of-the-art treatments. Whether you are visiting our office in Clinton, NJ, or our location in Bridgewater, NJ, we are dedicated to ensuring you receive the highest quality of service, compassion, and level of care you deserve.


Vein Treatments
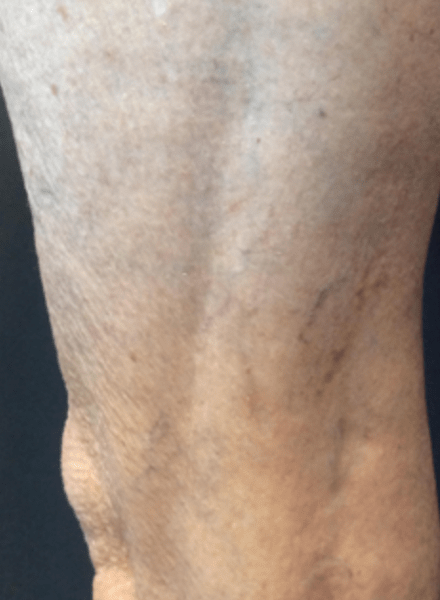
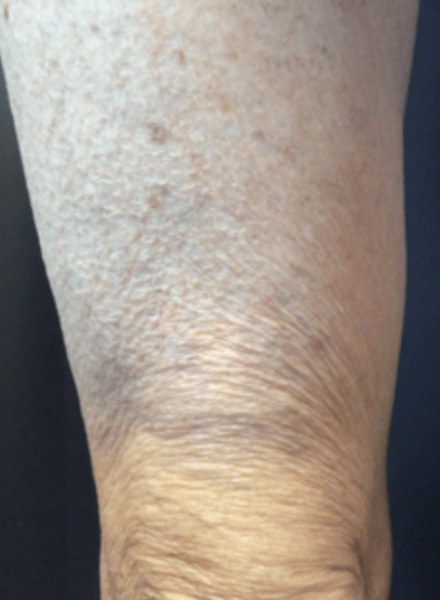
We offer a full range of the latest advancements in vein treatment for spider veins and varicose veins.
From addressing cosmetic concerns like red and blue web-like patterns to treating painful bulging and swelling caused by chronic venous insufficiency, our minimally invasive procedures, including Sclerotherapy, EVLT, and VenaSeal™, restore both the health and appearance of your legs.


Check out
Our Affiliations


Latest Blogs

Varicose veins develop when the ...

If you are dealing with bulging, ...

A venous ulcer can feel ...